Official Florida Hospital Template
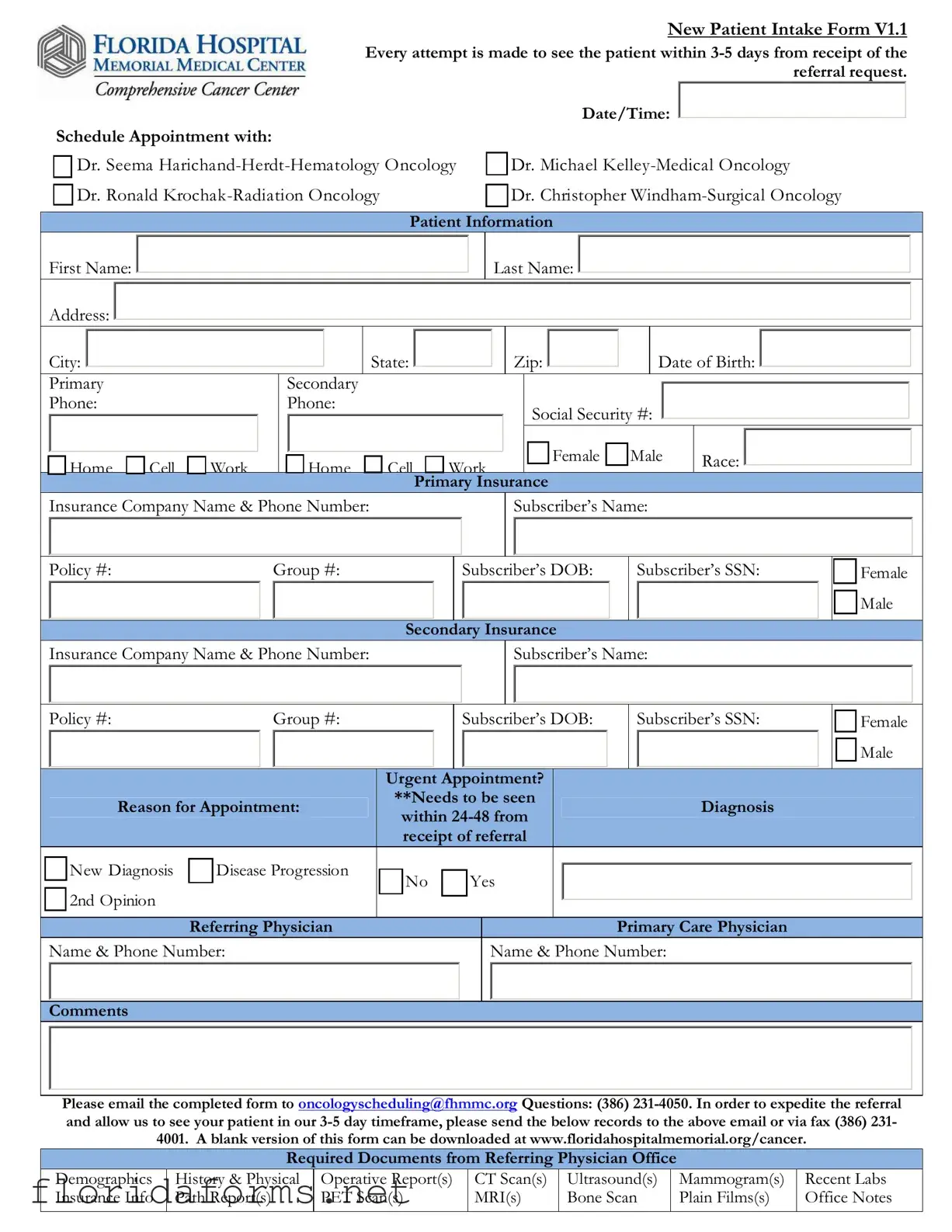
In the fast-paced world of healthcare, the efficiency and accuracy of patient intake processes can significantly impact the delivery of care, especially for new patients referred for specialized treatment. The Florida Hospital form for new patient intake is a comprehensive document designed to streamline the referral process, ensuring that patients requiring oncology services are seen by a specialist within 3-5 days from the receipt of their referral. This form captures essential patient information, including name, contact details, date of birth, social security number, and insurance data, which is critical for appointment scheduling and insurance verification. Patients are scheduled with one of several oncology specialists, depending on their diagnosis, which can range from Hematology Oncology, Medical Oncology, Radiation Oncology, to Surgical Oncology. The form distinguishes the urgency of appointments, catering specifically to those who need to be seen within 24-48 hours due to reasons like new diagnoses or disease progression. Furthermore, it requests detailed information about the referring and primary care physicians, enhancing coordination between different healthcare providers. To ensure a timely and effective referral process, referring physicians are asked to include supporting documents such as demographics, medical history, operative reports, and recent labs. This form exemplifies a well-orchestrated effort to facilitate timely access to specialized oncology services, underscoring the importance of comprehensive and coordinated patient care.
Example - Florida Hospital Form
New Patient Intake Form V1.1 Every attempt is made to see the patient within
Schedule Appointment with: |
|
Date/Time: |
|
|
|
|||
|
|
|
||||||
|
|
|
|
|
||||
|
|
Dr. Seema |
|
Dr. Michael |
||||
|
|
|
||||||
|
||||||||
|
||||||||
|
|
Dr. Ronald |
|
|
Dr. Christopher |
|||
|
|
|
|
|||||
|
|
|
|
|||||
Patient Information
First Name: 

Address: 
Last Name: 


|
City: |
|
|
|
|
State: |
|
|
|
|
Zip: |
|
|
|
|
|
|
Date of Birth: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
Primary |
|
Secondary |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Phone: |
|
Phone: |
|
|
|
|
Social Security #: |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Home |
Cell |
Work |
Home |
Cell |
Work |
Female |
Male |
Race: |
|
|
|
|
|
Primary Insurance |
|
|
|
|
|
Insurance Company Name & Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber’s Name: |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Policy #: |
|
|
|
Group #: |
|
|
|
|
|
|
|
Subscriber’s DOB: |
|
|
Subscriber’s SSN: |
|
|
Female |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Secondary Insurance |
|
|
|
|
|
|
|
|||||||||||||||
|
|
Insurance Company Name & Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber’s Name: |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Policy #: |
|
|
|
Group #: |
|
|
|
|
|
|
|
Subscriber’s DOB: |
|
|
Subscriber’s SSN: |
|
|
Female |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Urgent |
|
|
|
|
|
Appointment? |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
**Needs to be seen |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
Reason for Appointment: |
|
|
|
|
Diagnosis |
|
|
|
|
||||||||||||||||||||
|
|
|
|
within |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
receipt of referral |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
New Diagnosis |
|
Disease Progression |
|
No |
|
|
|
|
Yes |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
2nd Opinion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Referring Physician |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary Care Physician |
|
|
|
|
||||||
|
|
Name & Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
Name & Phone Number: |
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comments |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please email the completed form to oncologyscheduling@fhmmc.org Questions: (386)
|
|
|
|
|
|
|
|
|
|
|
|
Required Documents from Referring Physician Office |
|
|
|
||||
|
Demographics |
History & Physical |
Operative Report(s) |
CT Scan(s) |
Ultrasound(s) |
|
Mammogram(s) |
Recent Labs |
|
|
Insurance Info |
Path Report(s) |
PET Scan(s) |
MRI(s) |
Bone Scan |
|
Plain Films(s) |
Office Notes |
|
Patient Label
THIS SECTION TO BE COMPLETED BY THE CANCER CENTER SCHEDULER
PATIENT INFORMATION
|
First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name: |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
APPOINTMENT DATE/TIME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CARE NAVIGATORS NOTIFIED |
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Breast Care Navigator |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Appt Date: |
|
|
|
|
|
|
|
|
|
|
|
Appt Time: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lung Care Navigator |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
PATIENT AND APPOINTMENT ENTERED INTO SYSTEM |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
Radiation Oncology (Dr. Krochak) |
|
|
|
|
|
|
Dr. Harichand, Dr. Kelley, Dr. Windham |
|
|
|||||||||||||||||||||||||
|
MR # |
|
|
|
|
|
|
FIN# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Cerner Scheduling |
|
|
IMPAC |
|
|
|
ARIA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
PATIENT NOTIFIED |
|
|
|
|
|
|
|
|
NEW PATIENT PACKET GIVEN TO PT |
|
|
||||||||||||||||||||||||||||
|
Date/Time Patient Notified: |
|
|
|
CCC General Pt Packet |
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailed |
Date/Time: |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Spoke directly to patient |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Spoke with patients family |
|
|
|
|
|
|
|
|
|
|
Emailed |
Email Address |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
RECORDS RECEIVED FROM REFERRING PHYSICIAN |
|
|
|
|
|
|||||||||||||||||||||||||||
|
Date: |
|
|
|
|
|
|
|
|
|
|
Pathology Report |
|
|
|
Operative Report |
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Applicable Consultation Reports |
|
|
Bone Scan |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
History & Physical |
Most Recent Blood Work (Labs) |
|
CT Scan |
|
|
|||||||||||||||||||
|
Time: |
|
|
Initials: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PET Scan |
|
|
|
|
|
|
MRI |
|
|
Mammogram |
|
Ultrasound |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHART CREATED |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Radiation Oncology (Dr. Krochak) |
|
|
|
|
|
|
Dr. Harichand, Dr. Kelley, Dr. Windham |
|
|
|||||||||||||||||||||||||||||
|
Chart Label printed (Name & MRN) |
|
|
|
|
|
|
|
|
|
|
Chart Label printed (Name & DOB) |
|
|
|
|
|
|||||||||||||||||||||||
|
Facesheet & Labels printed from Cerner |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
Records in chart |
|
|
|
|
|
||||||||||||||||||||||||||||
|
Records in chart |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
CHART FORWARDED TO NURSING |
|
|
|
|
|
|
|
|
|
|
|
|
NURSING RECEIVED |
|
|
||||||||||||||||||||||||
|
Date/Time: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initials: |
|
|
|
|
|
Date/Time: |
|
|
|
|
|
Initials: |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Notes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
File Specifications
| Fact Name | Description |
|---|---|
| Form Version | The document is identified as New Patient Intake Form V1.1. |
| Appointment Timeliness | Efforts are made to schedule the patient within 3-5 days from receiving the referral request. |
| Contact Information | For completing and inquiries about the form, contact is directed through email to oncologyscheduling@fhmmc.org or by phone at (386) 231-4050. |
| Governing Law | The form is subject to Florida state laws, as it is used by a Florida-based hospital for patient intake in oncology scheduling. |
Instructions on Filling in Florida Hospital
Filling out hospital forms correctly is essential for ensuring your appointment and treatment start off smoothly. The Florida Hospital New Patient Intake Form is designed to gather all necessary information about you and your medical history, allowing healthcare providers to offer the best care possible. Here's a step-by-step guide to help you through the process, ensuring all information is accurate and submitted properly.
- Choose the appropriate specialist you need to see from the list provided and enter the preferred date and time for your appointment.
- Fill in your personal information, including your first and last name, address (city, state, zip), date of birth, and social security number.
- Provide your contact information, listing primary and secondary phone numbers. Make sure to indicate if it's a home, cell, or work number by checking the appropriate box.
- Specify your gender and race by selecting the appropriate options provided on the form.
- Under the Primary Insurance section, enter the insurance company name and phone number, the subscriber's name, policy and group numbers, the subscriber’s date of birth, and social security number. Indicate the subscriber’s gender.
- If applicable, repeat the process for your Secondary Insurance information.
- Mark whether an urgent appointment is needed and provide the reason for the appointment, such as a new diagnosis, disease progression, or a second opinion.
- Enter the referring physician’s and primary care physician's name and contact details, including their phone numbers.
- Check any additional comments that might help with your care or appointment scheduling.
- Email the completed form to oncologyscheduling@fhmmc.org, and contact them at (386) 231-4050 if you have any questions.
- Ensure that all required documents from the referring physician’s office—such as demographic information, history & physical reports, relevant scans and tests, and insurance information—are sent to the email or fax number provided on the form.
After submitting your form and the required documents, the cancer center scheduler will complete their section, enter your information into their system, and notify the corresponding care navigators. They will also inform you about the appointment details and give you a new patient packet. Please remember to follow up if you haven't received confirmation of your appointment within the expected timeframe.
Understanding Florida Hospital
What is the purpose of the New Patient Intake Form V1.1?
The New Patient Intake Form V1.1 is designed to gather all necessary patient information to schedule an appointment at the Florida Hospital for various oncology specialists. It ensures that the patient can be seen within 3-5 days from the receipt of the referral request, helping to expedite the process for urgent care needs, such as new diagnoses or disease progression.
How can I choose a specific oncologist from the provided list?
On the form, you have the option to schedule an appointment with one of four oncology specialists by indicating your choice under the "Schedule Appointment with" section. Each specialist focuses on a different area of oncology, allowing you to select the one that best fits your medical needs.
What information is required for the patient section of the form?
The patient section of the form requires comprehensive personal and contact information, including first and last name, address, phone numbers, social security number, date of birth, gender, race, and detailed insurance information. This ensures that the hospital can effectively communicate with the patient and process insurance claims appropriately.
Can I mark an appointment as urgent and what does it mean?
Yes, you can indicate whether an appointment is urgent by selecting "Yes" under the "Urgent Appointment?" section. An urgent appointment means that the patient needs to be seen within 24-48 hours due to a critical condition such as a new diagnosis or significant disease progression. This feature helps prioritize the scheduling of appointments for patients with immediate care needs.
What steps should be followed after completing the form?
After filling out the form, you should email it to oncologyscheduling@fhmmc.org. Additionally, referring physicians are asked to send the patient's medical records, including demographic information, history & physical, recent labs, and any relevant reports or scans, to the same email or via fax. This comprehensive approach ensures that the oncology team has all necessary information to provide the best possible care during the scheduled appointment.
Common mistakes
When filling out the Florida Hospital New Patient Intake Form, mistakes can complicate or delay the process of scheduling a much-needed appointment. To ensure that the form is completed accurately and efficiently, avoiding these common errors is crucial:
Not verifying the appointment section - Sometimes, in the rush to fill out the personal information, the appointment section at the top of the form gets overlooked. It is important to confirm the appointment details, including the date and time, and the specific doctor you are scheduled to see.
Incorrect or incomplete patient information - Providing accurate patient details, including first and last name, address, and especially the date of birth and social security number, is vital. Mistakes here can lead to insurance claims issues or delays in receiving care.
Omitting contact numbers - The form requests both primary and secondary phone numbers with specifications for home, cell, or work numbers. Leaving these fields incomplete might hinder the hospital staff's ability to reach out for appointment confirmations or necessary follow-ups.
Insurance information inaccuracies - Accurately detailing primary and secondary insurance information, including company name, policy number, and subscriber details, is crucial. Any errors or omissions can create billing issues or even affect your eligibility for some services.
Missing urgency and referral details - Not specifying whether the appointment is urgent or failing to provide complete referral details, including the referring physician's information and reason for the appointment, can result in scheduling mishaps. Especially for urgent needs, articulating the immediacy can expedite appointment scheduling.
To avoid these common pitfalls, it’s encouraged to double-check all the information before submitting the form. Taking an extra moment to verify details can make a significant difference in how quickly and smoothly the appointment process unfolds.
Documents used along the form
In the realm of medical treatment and care, particularly within hospital settings in Florida, a plethora of forms and documents play crucial roles in ensuring the seamless operation of patient care services. Among these, the Florida Hospital form, referred to as the "New Patient Intake Form V1.1", is pivotal for patient intake processes. However, this form is just the beginning. There's a suite of additional documents often used alongside it, each serving a distinct and important function in the patient care continuum. Here's a closer look at some of these key documents:
- Advanced Healthcare Directive (Living Will): This document allows patients to outline their preferences for medical treatment in scenarios where they are unable to make decisions for themselves. It includes conditions under which life support should be initiated or withheld.
- Medical Power of Attorney (POA): Assigns a healthcare proxy, who is authorized to make healthcare decisions on behalf of the patient when they are unable to communicate their medical wishes themselves.
- HIPAA Authorization Form: Ensures compliance with the Health Insurance Portability and Accountability Act by obtaining patient consent to share their medical information for treatment purposes, billing, and healthcare operations.
- Medication List: A comprehensive record of all medications a patient is currently taking, including doses and frequency. This is crucial for avoiding potential drug interactions and ensuring that the healthcare team is fully informed.
- Insurance Verification Form: Used to confirm a patient's insurance coverage details, this form assists in the billing process and ensures that services provided are covered under the patient’s health plan.
- Release of Information Form: Allows for the transfer of medical records and information between different healthcare providers or institutions, facilitating continuity of care.
- Patient Rights and Responsibilities: Informs patients of their rights and responsibilities while receiving care within the healthcare facility, promoting an understanding of mutual expectations.
- Financial Agreement or Policy Acknowledgment Form: This document outlines the financial policies of the healthcare facility, including payment expectations, billing procedures, and information about financial assistance if necessary.
In addition to the Florida Hospital New Patient Intake Form, these documents play an integral role in the patient care process. They ensure clear communication between patients and healthcare providers, protect patient rights, and enable efficient operation of healthcare facilities. Each document, with its specific purpose, contributes to creating a comprehensive and patient-centered approach to healthcare.
Similar forms
Patient Registration Forms: Similar to the Florida Hospital form, Patient Registration Forms gather essential demographic and contact information from patients, including name, address, and phone numbers. This ensures the healthcare provider has accurate records for communication and billing purposes.
Medical History Forms: These forms are designed to collect a patient's medical history, much like the section in the Florida Hospital form that requests information on diagnosis and reason for the appointment. Both types of documents are vital for informing healthcare providers about past and current health issues, ensuring appropriate care.
Insurance Verification Forms: The section in the Florida Hospital form that requests primary and secondary insurance information resembles Insurance Verification Forms. These documents are crucial for determining the coverage and ensuring the healthcare provider receives payment for services rendered.
Referral Forms: Just like the portion of the Florida Hospital form that asks for referral details, Referral Forms are used to document and formalize the process of one healthcare provider referring a patient to another for expert consultation or treatment, specifying the reason for the referral and urgency.
Consent for Treatment Forms: Although not directly mentioned, the New Patient Intake Form implies a level of consent for the scheduling and facilitation of oncological care. Consent for Treatment Forms explicitly collect patient or guardian consent for procedures and treatments, addressing legal and ethical requirements.
Emergency Contact Forms: Gathering contact information for situations that require urgent communication with someone close to the patient is a commonality shared with the section in the Florida Hospital form that collects phone numbers. These details are crucial in case of emergencies.
Appointment Scheduling Forms: The Florida Hospital form schedules an appointment, specifying dates and times with various specialists. This is akin to general Appointment Scheduling Forms used in many healthcare settings to organize and record upcoming patient visits.
Privacy Notice Acknowledgment Forms: While the Florida Hospital form is primarily focused on gathering information and scheduling, it is part of a larger practice of informing patients about how their information is used, resonating with Privacy Notice Acknowledgment Forms that ensure patients are aware of their rights under privacy laws like HIPAA.
Advance Directive Forms: While not directly related to intake or scheduling, Advance Directive Forms, like parts of the Florida Hospital form, are essential in the broader context of patient care and decision-making, documenting patients' wishes regarding healthcare decisions in future scenarios where they may be unable to communicate.
Dos and Don'ts
Filling out hospital forms can be a crucial step in ensuring you get the care you need. When dealing with the Florida Hospital New Patient Intake Form, here are some essential dos and don'ts to keep in mind:
Things You Should Do:
Double-check all personal information (such as your name, address, and date of birth) for accuracy to avoid any issues with your care or records.
Ensure that your insurance details are up-to-date and correctly entered, including the policy number and insurance company name.
Clearly indicate the necessity of an urgent appointment if your situation requires immediate attention, specifying the reason for the urgency.
Provide comprehensive contact information, including a primary and secondary phone number, to facilitate easy communication.
Things You Shouldn't Do:
Don't leave sections blank unless they truly do not apply to your situation. If unsure, it's better to provide too much information than too little.
Avoid using nicknames or abbreviations. Use your legal name and the full names of your insurance providers to prevent confusion.
Do not forget to list a secondary insurance if you have one. This can be important for covering costs that your primary insurance does not.
Never hesitate to ask for help if you're unsure about what information is required. Contact the provided number for any questions to ensure the form is completed accurately.
Misconceptions
Common misconceptions about the Florida Hospital form often lead to confusion for patients and healthcare providers alike. Addressing these misunderstandings is crucial for ensuring a seamless and efficient intake process. Here are several clarifications:
- 1. "The form exclusively serves for scheduling appointments." While scheduling is a significant component, the form also plays a vital role in gathering comprehensive patient information, ensuring proper care navigation, and facilitating the expedited sharing of medical records.
- 2. "Insurance details are optional." On the contrary, providing primary and secondary insurance information is essential. This enables the hospital to verify coverage and reduce the administrative burden on patients and their families, ensuring treatments are not delayed due to financial verification needs.
- 3. "The form must be faxed." Despite fax being an option, the form highlights the efficacy of email communication. By emailing the completed form to oncologyscheduling@fhmmc.org, referrals are expedited, aligning with the goal to see patients within 3-5 days from receipt of a referral.
- 4. "The form is only for new patients." Although it's indeed a New Patient Intake Form, it includes sections for urgent appointments and diagnosis, serving both new and existing patients who may require immediate attention or a new consultation due to changes in their diagnosis or disease progression.
- 5. "All patients are seen within 3-5 days." This timeframe is an attempt, not a guarantee. While every effort is made to see patients quickly, varying factors such as the patient’s medical urgency, physician availability, and the completeness of the required documents can affect actual scheduling.
- 6. "The patient must complete all documentation." Both the referring physician's office and the patient contribute information. Necessary documents from the referring physician, such as demographics and medical history, are crucial for a comprehensive understanding and treatment plan. The form delineates responsibilities to streamline the intake process.
Dispelling these misconceptions ensures patients and healthcare providers approach the Florida Hospital New Patient Intake Form with accurate expectations, fostering a smoother healthcare journey for all parties involved.
Key takeaways
Completing and utilizing the Florida Hospital New Patient Intake Form is a vital step in ensuring that new patients are promptly and efficiently integrated into the Florida Hospital care system. Here are some key takeaways that highlight the importance of this process:
- The form aims to schedule appointments for new patients within 3-5 days of receiving the referral, underlining the hospital's commitment to timely care, especially in departments such as Hematology Oncology, Medical Oncology, Radiation Oncology, and Surgical Oncology.
- Patient information must be meticulously filled out, including basic details like name, address, date of birth, and contact numbers, as well as the social security number and gender, echoing the necessity of accurate records for ensuring proper care and communication.
- It's mandatory to specify the primary and secondary insurance details, including the subscriber’s name, policy and group numbers, and subscriber's social security number, underscoring the significance of financial arrangements in healthcare services.
- The form asks whether the appointment is urgent, with options to indicate if the patient needs to be seen within 24-48 hours, demonstrating the hospital’s responsiveness to critical cases.
- Reasons for appointment are to be clearly stated, including whether it’s for a new diagnosis, disease progression, a second opinion, or other reasons, ensuring that the healthcare provider is prepared for the patient’s specific needs.
- Information about the referring and primary care physician must be provided, facilitating a seamless communication and coordination among the medical professionals involved in the patient’s care.
- Instructions for the referring physician's office to expedite the referral process by providing essential documents highlight the collaborative effort necessary for effective patient care.
- The form includes a section for internal use by the cancer center scheduler and care navigators, indicating an organized approach to managing patient appointments and care navigation.
- Notification and communication channels with the patient or their family are documented, emphasizing the importance of keeping the patient informed and involved in their care process.
- A list of required documents from the referring physician underlines the comprehensive evaluation needed for an accurate and complete medical assessment, comprising demographics, history and physical, reports of operative interventions, and various scans and tests results.
By meticulously following these guidelines, healthcare providers can ensure that all necessary information is accurately captured and communicated, supporting the delivery of high-quality care tailored to each patient's unique needs.
Popular PDF Templates
Florida Ucc1 - Completion of faculty credentials section ensures instructors meet minimum teaching standards.
Florida Court - Highlight of the requirement to notify other parties of the motion hearing at least five business days in advance to avoid dismissal or striking of the motion.
Income Withholding Order Florida - Illustrates the means through which employees can contest wrongful employment actions related to income withholding, empowering affected workers.