Official First Report Of Injury Florida Template
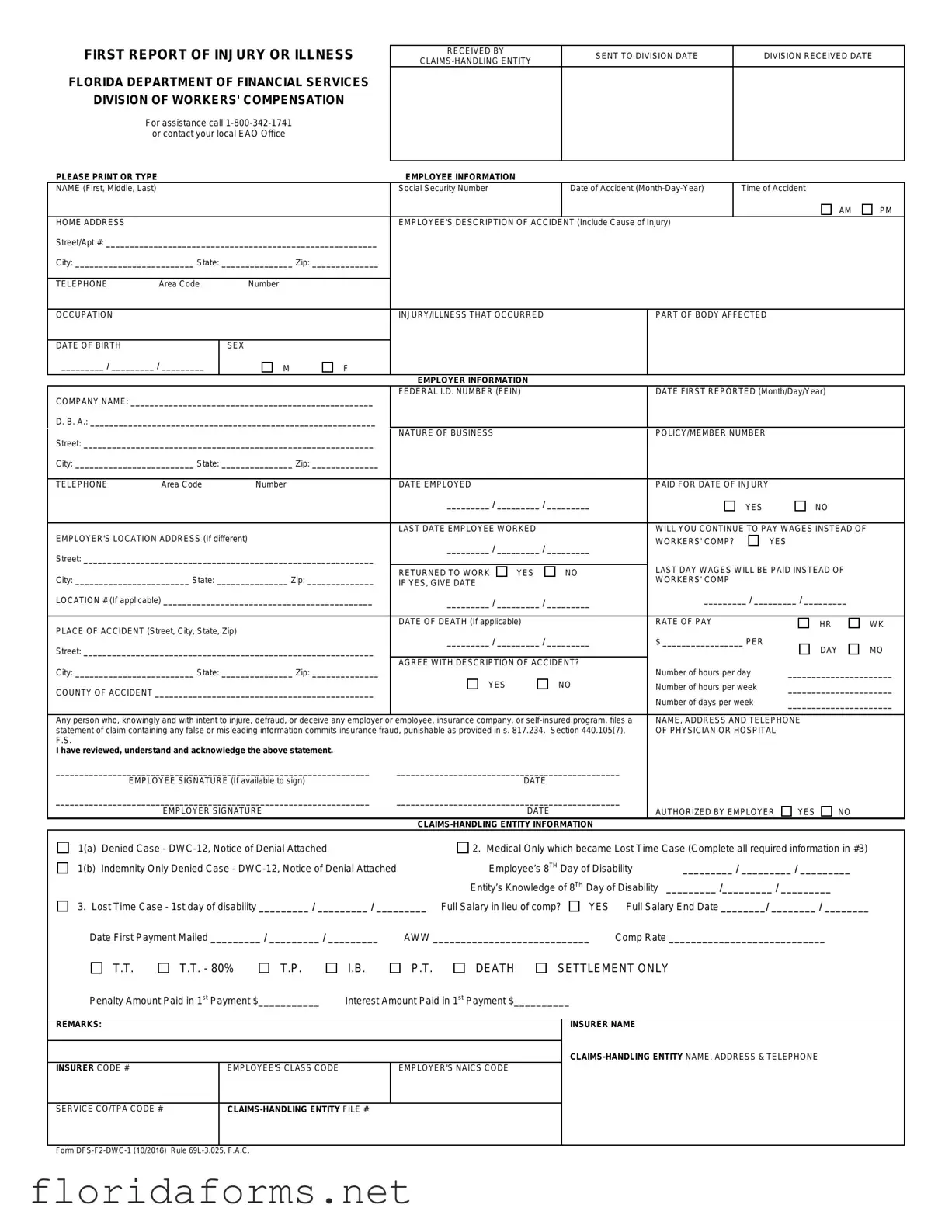
When an employee in Florida suffers an injury or illness due to their work, the process of reporting the incident officially begins with the “First Report of Injury or Illness” form, a critical document facilitated by the Florida Department of Financial Services, Division of Workers' Compensation. This form, essential for initiating a workers' compensation claim, requires meticulous detail, including employee information such as name, social security number, and a thorough description of the accident and the injury or illness incurred. It also encompasses employer information, including company name, federal ID number, and the nature of the business, alongside specific details about the accident, such as the date, time, and location where the incident occurred. Moreover, it captures data on whether the employee had to stop working, if the employer will continue to pay wages, and details about the physician or hospital that provided initial treatment. A noteworthy aspect of this form is its role in declaring an employee's cessation of work and the subsequent financial adjustments and medical treatment implications. The form serves as a foundational document in the workers' compensation claims process, signifying the commencement of potential financial and medical support for the injured or ill employee, all underlined with an admonition against insurance fraud. The intensive detail it requires underscores its significance in the efficient management and resolution of workers' compensation claims. This comprehensive approach ensures accuracy in information, a necessity for both protecting the rights of the employee and the obligations of the employer under Florida law.
Example - First Report Of Injury Florida Form
FIRST REPORT OF INJURY OR ILLNESS
FLORIDA DEPARTMENT OF FINANCIAL SERVICES
DIVISION OF WORKERS' COMPENSATION
For assistance call
PLEASE PRINT OR TYPE
RECEIVED BY |
SENT TO DIVISION DATE |
DIVISION RECEIVED DATE |
|
|
|
||
|
|
|
EMPLOYEE INFORMATION
NAME (First, Middle, Last) |
|
|
|
Social Security Number |
|
|
Date of Accident |
|
Time of Accident |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
HOME ADDRESS |
|
|
|
EMPLOYEE'S DESCRIPTION OF ACCIDENT (Include Cause of Injury) |
|
|
|
|
|||||
Street/Apt #: _________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
Area Code |
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
OCCUPATION |
|
|
|
INJURY/ILLNESS THAT OCCURRED |
|
|
PART OF BODY AFFECTED |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
SEX |
|
|
|
|
|
|
|
|
|
|
|
_________ / _________ / _________ |
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER INFORMATION |
|
|
|
|
|
|
|
|
|
COMPANY NAME: ___________________________________________________ |
FEDERAL I.D. NUMBER (FEIN) |
|
|
DATE FIRST REPORTED (Month/Day/Year) |
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||
D. B. A.: ____________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
Street: _____________________________________________________________ |
NATURE OF BUSINESS |
|
|
|
POLICY/MEMBER NUMBER |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
TELEPHONE |
Area Code |
Number |
|
DATE EMPLOYED |
|
|
|
PAID FOR DATE OF INJURY |
|
|
|
||
|
|
|
|
_________ / _________ / _________ |
|
|
YES |
|
NO |
|
|||
|
|
|
|
|
|
|
|
|
|
||||
EMPLOYER'S LOCATION ADDRESS (If different) |
|
LAST DATE EMPLOYEE WORKED |
|
|
WILL YOU CONTINUE TO PAY WAGES INSTEAD OF |
|
|||||||
|
_________ / _________ / _________ |
WORKERS' COMP? |
|
YES |
|
||||||||
|
|
|
|
|
|
||||||||
Street: _____________________________________________________________ |
|
|
|
|
|
|
|||||||
|
|
|
|
LAST DAY WAGES WILL BE PAID INSTEAD OF |
|
||||||||
|
|
|
|
RETURNED TO WORK |
YES |
|
NO |
|
|||||
City: ________________________ State: _______________ Zip: ______________ |
|
WORKERS' COMP |
|
|
|
|
|||||||
IF YES, GIVE DATE |
|
|
|
|
|
|
|
||||||
LOCATION # (If applicable) ____________________________________________ |
_________ / _________ / _________ |
_________ / _________ / _________ |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
RATE OF PAY |
|
|
|
|
||
PLACE OF ACCIDENT (Street, City, State, Zip) |
|
DATE OF DEATH (If applicable) |
|
|
|
|
HR |
WK |
|||||
|
|
|
|
|
|
|
|
|
|||||
|
_________ / _________ / _________ |
$ _________________ PER |
|
|
|
||||||||
Street: _____________________________________________________________ |
|
DAY |
MO |
||||||||||
|
|
|
|
|
|
|
|
||||||
City: _________________________ State: _______________ Zip: ______________ |
AGREE WITH DESCRIPTION OF ACCIDENT? |
Number of hours per day |
______________________ |
||||||||||
|
|
|
|
||||||||||
COUNTY OF ACCIDENT ______________________________________________ |
YES |
|
NO |
Number of hours per week |
______________________ |
||||||||
|
|
|
|
Number of days per week |
______________________ |
||||||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|||||||||
Any person who, knowingly and with intent to injure, defraud, or deceive any employer or |
employee, insurance company, or |
NAME, ADDRESS AND TELEPHONE |
|
||||||||||
statement of claim containing any false or misleading information commits insurance fraud, punishable as provided in s. 817.234. Section 440.105(7), |
OF PHYSICIAN OR HOSPITAL |
|
|||||||||||
F.S. |
|
|
|
|
|
|
|
|
|
|
|
|
|
I have reviewed, understand and acknowledge the above statement.
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYEE SIGNATURE (If available to sign) |
DATE |
|
|
|
|
|
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYER SIGNATURE |
DATE |
|
AUTHORIZED BY EMPLOYER |
YES |
NO |
|
|
|
|
|
|
|
||
1(a) |
Denied Case - |
2. Medical Only which became Lost Time Case (Complete all required information in #3) |
|||||
1(b) |
Indemnity Only Denied Case - |
Employee’s 8TH Day of Disability |
_________ / _________ / _________ |
||||
|
|
Entity’s Knowledge of 8TH Day of Disability |
_________ /_________ / _________ |
|
|||
3. Lost Time Case - 1st day of disability _________ / _________ / _________ Full Salary in lieu of comp? |
YES |
Full Salary End Date ________/ ________ / ________ |
|||||
Date First Payment Mailed _________ / _________ / _________ |
AWW ____________________________ |
Comp Rate ____________________________ |
|
||||
T.T.
T.T. - 80%
T.P.
I.B.
P.T.
DEATH
SETTLEMENT ONLY
Penalty Amount Paid in 1st Payment $___________ |
Interest Amount Paid in 1st Payment $__________ |
REMARKS:
INSURER CODE # |
EMPLOYEE'S CLASS CODE |
EMPLOYER'S NAICS CODE |
|
|
|
INSURER NAME
SERVICE CO/TPA CODE #
Form
The collection of the social security number on this form is specifically authorized by Section 440.185(2), Florida Statutes. The social security number will be used as a unique identifier in Division of Workers' Compensation database systems for individuals who have claimed benefits under Chapter 440, Florida Statutes. It will also be used to identify information and documents in those database systems regarding individuals who have claimed benefits under Chapter 440, Florida Statutes, for internal agency tracking purposes and for purposes of responding to both public records requests and subpoenas that require production of specified documents. The social security number may also be used for any other purpose specifically required or authorized by state or federal law.
File Specifications
| Fact Name | Description |
|---|---|
| Form Identifier | FIRST REPORT OF INJURY OR ILLNESS FLORIDA |
| Governing Body | FLORIDA DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS' COMPENSATION |
| Assistance Information | For assistance call 1-800-342-1741 or contact your local EAO Office |
| Reporting Requirement | Mandatory for initiating Workers' Compensation claims |
| Governing Law | Rule 69L-3.025, F.A.C. |
| SSN Collection Authorization | Section 440.185(2), Florida Statutes authorizes collection of social security number. |
| Usage of Social Security Number | Used as a unique identifier in database systems and for internal tracking. |
| Fraud Warning Statement | Includes a warning about the criminal penalties for filing a false or misleading claim. |
| Signature Requirement | Must be reviewed, understood, and acknowledged by employee and employer. |
Instructions on Filling in First Report Of Injury Florida
Filling out the First Report of Injury or Illness form is an essential step if you've been injured or fallen ill due to your job in Florida. This document notifies the Florida Department of Financial Services' Division of Workers' Compensation about your situation, so it's important to complete it accurately and promptly. Follow these step-by-step instructions to ensure you fill out the form correctly.
- Start by entering the date you received the form and the date you're sending it to the Division in the designated spots at the top of the form.
- Provide the Claims-Handling Entity information, including their name, if known.
- Under the Employee Information section, write your full name, social security number, date, and time of the accident. Specify AM or PM for the time.
- Enter your home address, including street, city, state, and zip code, along with your telephone number.
- Detail your occupation, the injury or illness that occurred, and the part of the body affected. Also, include your date of birth and gender.
- In the Employer Information section, fill in your company's name, Federal ID Number (FEIN), and if applicable, a Doing Business As (D.B.A.) name.
- Add the nature of the business, policy/member number, employer's address (street, city, state, zip code), and telephone number.
- Provide the date you first reported the injury, your date of employment, and check whether you were paid for the date of the injury.
- Fill in details about the last date you worked, if wages will continue instead of workers' compensation, and if yes, when this will end.
- State whether you've returned to work, and if so, the date of return.
- Indicate your rate of pay and place of accident, including specific details about the location (street, city, state, zip code).
- If applicable, fill in the date of death.
- Confirm whether you agree with the description of the accident, your work schedule details, and if any wages will be continued instead of compensation.
- Provide the name, address, and telephone of the physician or hospital treating you.
- Employee Signature: Sign and date the form if you're available to do so.
- Employer Information: The employer or authorized representative should sign and date the form, indicating whether they agree with the information provided.
- Under the Claims-Handling Entity Information, include details if the case was denied, if it's a medical-only case that became a lost-time case, include all relevant dates, compensation rates, and any other required information.
- Insert remarks if necessary, along with insurer code, employee class code, employer's NAICS code, insurer, and claims-handling entity name, address, and telephone number.
After you've completed all the necessary sections of the form, review it to ensure that all the information provided is accurate and true. Submit the form as directed by your employer or insurance representative. This document is crucial for initiating your worker's compensation claim, so it's important to fill it out as soon as possible after your injury or diagnosis. Your prompt action can help to ensure that you receive any benefits you're entitled to without unnecessary delays.
Understanding First Report Of Injury Florida
What is the First Report of Injury or Illness Form in Florida?
The First Report of Injury or Illness Form, known as Form DFS-F2-DWC-1, is a critical document in the Florida workers' compensation process. It's used to report an employee's injury or illness that is believed to be work-related. This form initiates the claim process with the Florida Department of Financial Services, Division of Workers' Compensation. It collects essential information about the employee, the employer, the nature of the injury or illness, and details about the accident or cause of the illness. This form serves as the first formal notification to the state about a workplace injury, enabling the affected employee to potentially receive benefits.
Who needs to fill out the First Report of Injury or Illness Form?
Typically, this form is filled out by the employer on behalf of the employee who has suffered a work-related injury or illness. It's the employer's responsibility to accurately document the incident and any initial treatment the employee received. The process usually involves gathering detailed information from the injured or ill employee to ensure the form is completed comprehensively. Employers should note that even if an injury seems minor, documenting it formally is always a prudent measure to protect both the employee's rights and the employer's interests. Employees should ensure their employer is aware of any work-related injuries or illnesses that might necessitate filling out this form.
How does the First Report of Injury or Illness Form affect a worker's compensation claim?
Submitting the First Report of Injury or Illness Form is the first step in the workers' compensation claim process in Florida. The information provided on this form is used by the Florida Division of Workers' Compensation to open a case and start the review process. This form's details allow for an assessment of the claim, determining eligibility for workers' compensation benefits, and if eligible, what benefits are appropriate based on the injury or illness reported. It’s essential for the form to be filled out accurately and completely, as missing or incorrect information can delay the processing of a claim or affect the benefits an employee receives.
What happens after the First Report of Injury or Illness Form is submitted?
After the First Report of Injury or Illness Form is submitted to the Florida Division of Workers' Compensation, a claims-handling entity, often an insurance company, will review the claim. This review includes assessing the validity of the claim, the extent of the injury or illness, and determining the appropriate benefits under Florida law. The employee may be asked to provide additional information or documentation, and in some cases, undergo a medical examination. If approved, the claims process moves forward to include benefits like medical treatment coverage, reimbursement for lost wages, and other necessary compensations. If the claim is denied or if there are disputes about the benefits, both employers and employees have the right to challenge the decision through a legal process.
Common mistakes
Filling out the First Report of Injury or Illness form for Florida's Department of Financial Services Division of Workers' Compensation presents a crucial step in the workers' compensation claim process. However, individuals often make mistakes when completing this form, potentially complicating their claim. Here are seven common errors:
- Not providing complete employee information, including the full name and social security number, which are essential for processing the claim and identifying the individual in the workers' compensation database systems.
- Failing to accurately describe the accident, including the cause of injury. A detailed and clear description is crucial for a proper understanding of the circumstances surrounding the accident.
- Omitting the exact date and time of the accident, which are necessary for verifying the claim and determining eligibility for workers' compensation benefits.
- Incorrectly identifying the body part affected by the injury or illness. Precise information helps in assessing the claim and determining the appropriate medical treatment and compensation.
- Providing incomplete employer information, such as the company name or Federal Identification Number (FEIN). This information is vital for processing the claim and verifying employment.
- Not accurately reporting the employment and injury details, including the date employed, wages, and location of the accident. These details are crucial for calculating compensation rates and benefits.
- Signing the form without reviewing the fraud warning or understanding the implications of providing false information, which is a punishable offense.
By avoiding these common mistakes, individuals can ensure that their First Report of Injury or Illness is correctly filled out, facilitating a smoother process in claiming workers' compensation benefits.
Documents used along the form
When filing a First Report of Injury or Illness in Florida, a comprehensive and well-documented approach ensures that all parties involved receive accurate and timely support and benefits. Aside from the primary form that initiates the reporting process under the Division of Workers' Compensation, several other documents and forms often accompany this initial submission to facilitate a thorough understanding and processing of the claim. Each document serves a specific purpose in the context of a workers' compensation claim, helping to paint a full picture of the incident, the affected employee, and the steps being taken by the employer and insurance carrier.
- DWC-12, Notice of Denial: This form is utilized when a claim is denied by the claims-handling entity. It outlines the reasons for denial and provides essential information on how the employee can contest this decision.
- Employee’s Wage Statement: Helps in determining the correct compensation rate for the injured employee by providing a detailed record of the wages earned prior to the injury.
- Physician’s Report: Completed by the attending healthcare provider, this document details the employee's medical condition, the treatment received, and the prognosis, which aids in evaluating the claim and planning further medical care.
- Mileage Reimbursement Form: Allows employees to request reimbursement for travel expenses related to medical appointments or treatments as a result of the work-related injury.
- Release of Medical Records Form: Authorizes the disclosure of the employee’s medical information pertinent to the claim, facilitating proper assessment and processing by the insurer or employer.
- Employee Claim Form DWC-1: Though this is the initial form, in some cases, it might be necessary to resubmit or provide additional information as the claim progresses.
- Return to Work Form: Filled out by the healthcare provider, it indicates when and under what conditions the employee can return to work, which is crucial for planning and accommodations.
- Death Certificate: In the unfortunate event of a fatality, this certificate is necessary to process claims for death benefits.
Together, these documents contribute to a well-rounded and legally sound worker's compensation claim. They ensure that all procedural requirements are met and facilitate a more seamless transition for the injured employee from injury through to recovery and, if possible, a return to work. By diligently completing and submitting these forms, employers and employees help maintain compliance with Florida's workers' compensation laws while ensuring that the rights and well-being of all parties are upheld.
Similar forms
- Workers' Compensation Claim Form
- OSHA Form 300: Log of Work-Related Injuries and Illnesses
- Employer’s First Report of Injury or Fatality (Various State Versions)
- Accident Incident Report
- Employee’s Claim for Workers’ Compensation Benefits
- Notice of Occupational Disease and Claim for Compensation
- Insurance Claim Form
- Personal Injury Claim Form
This form, generally known in various states beyond Florida, is similar because it collects critical information following a workplace injury or illness. Like the First Report of Injury form in Florida, it includes details about the employee, the injury or illness sustained, employer information, and the circumstances surrounding the incident. Both forms are essential for initiating the claims process for workers' compensation benefits.
While the OSHA Form 300 is a log rather than a single incident report, its purpose aligns closely with that of the First Report of Injury form. It records work-related injuries and illnesses, detailing the nature and severity of each case. Both documents are crucial for workplace safety and health compliance, helping track the incidence and causes of workplace injuries and illnesses.
Many states have their versions of a first report for workplace injuries or fatalities, which serve a similar function to Florida's form. These documents are the initial step in notifying relevant state authorities and insurance entities about an employee injury or death, providing details such as employee information, injury specifics, and employer details. The core aim is to ensure the injured party receives appropriate workers' compensation benefits.
This type of report is used by organizations to document any incident or accident occurring on their premises, not limited to employee injuries. Its similarity to the First Report of Injury Florida form lies in its detailed account of the incident, including when, where, and how the incident took place, alongside personal details of those involved. Both forms are foundational to subsequent investigative and compensatory processes.
This document is similar to Florida's First Report of Injury or Illness form because it begins the process for an employee to claim workers' compensation benefits following an injury or illness. It typically includes details about the employee's injury or illness, employment information, and the treatment received. Both are pivotal in the compensation claim process, ensuring the injured or ill employee seeks and receives the benefits they are entitled to.
This document is used for reporting occupational diseases rather than injuries, which can be gradual or long-term conditions resulting from work activities or exposures. Like the First Report of Injury or Illness, it includes detailed information about the claimant, the condition complained of, and employment details, playing a critical role in the process to obtain compensation and benefits for occupational diseases.
Insurance claim forms, particularly those related to health, accident, or disability insurance, share similarities with the First Report of Injury Florida form. These forms are used to report an incident or condition to the insurance company to initiate a claim for benefits. They require detailed information about the incident (or health condition), the claimant, and coverage details, aiming to document the occurrence and basis for the claim comprehensively.
This form is used in various legal settings where an individual seeks compensation for injuries sustained due to someone else's negligence or fault. Like the First Report of Injury or Illness, it gathers information about the injury, how it occurred, and the impact on the individual’s life. Both are essential in the process of seeking redress and compensation for injuries, albeit in different contexts.
Dos and Don'ts
When filling out the First Report of Injury or Illness form for the Florida Department of Financial Services Division of Workers' Compensation, there are specific dos and don'ts to ensure the process is completed accurately and effectively. Adhering to these guidelines can help avoid delays or issues in processing the claim.
What You Should Do:
Ensure all information is printed or typed clearly to avoid any misunderstandings or processing delays caused by illegible handwriting.
Double-check the accuracy of all provided information, including the employee’s social security number, date of the accident, and the detailed description of the accident and injury. Accurate information is critical for the claims process.
Include a comprehensive employee description of the accident, specifying the cause of injury. This helps in establishing the context and circumstances surrounding the incident.
Verify the date of the accident and the time of the accident with precision, as this information can be crucial for validating the claim.
Provide the correct contact information for the physician or hospital that provided care to ensure the claims processing entity can verify the medical information if necessary.
Review the completed form for completeness and accuracy before submission to guarantee all required fields are filled out. This can prevent unnecessary back-and-forth and expedite the claim process.
What You Shouldn't Do:
Do not leave mandatory fields empty. An incomplete form may result in the rejection of the claim or significant delays in processing.
Avoid assuming details or making guesses about information you’re unsure of—especially concerning the employee’s description of the accident and the resultant injury or illness.
Do not forget to include the signature and date at the bottom of the form. An unsigned form may be considered invalid.
Resist the temptation to submit the form without reviewing the insurance fraud warning provided. Understanding the implications of submitting false or misleading information is essential.
Do not use the social security number for any other purposes than those authorized by Section 440.185(2), Florida Statutes, respecting privacy and legal guidelines.
Avoid delays in submitting the form after the incident. Prompt submission is key to ensuring timely processing and support for the injured employee.
By following these dos and don'ts, you can help ensure that the First Report of Injury or Illness form is filled out accurately and effectively, aiding the quick resolution of the claim.
Misconceptions
Misconception 1: The First Report of Injury Form is Only Necessary if the Injury is Severe
Many people mistakenly believe that the First Report of Injury or Illness form (DWC-1) needs to be completed only if the injury sustained by the employee is severe. In reality, this form should be filled out and submitted for any injury or illness that occurs in the workplace, regardless of severity. It initiates the workers’ compensation process, ensuring the employee can receive appropriate medical attention and any potential compensation benefits without unnecessary delay.
Misconception 2: The Employee is Responsible for Filing the Form
It's a common misunderstanding that the injured employee is the one who needs to file the First Report of Injury form. However, it is actually the employer's responsibility to complete and submit this form to the Division of Workers' Compensation in Florida. While the injured worker is responsible for reporting their injury or illness to their employer, the employer must take it from there by documenting the incident on this form and handling its submission.
Misconception 3: Filing the Form is the Same as Filing a Workers' Compensation Claim
Some believe that submitting the First Report of Injury or Illness form is equivalent to filing a workers' compensation claim. This is not accurate. This form merely documents the occurrence of an injury or illness. Filing an actual claim for workers' compensation benefits is a separate process that might require additional forms and steps before an employee can receive benefits. This form is a crucial step but not the only one in the workers' compensation claim process.
Misconception 4: The Form can Only be Submitted in Paper Form
With the advancements in digital technology and efforts to streamline workers' compensation processes, there's a misconception that the First Report of Injury form can only be submitted in paper form. However, many states, including Florida, allow or even prefer digital submission of this form. This digital option makes it easier and faster for employers to comply with reporting requirements, helping to expedite the review and processing of the worker's compensation claim.
Key takeaways
When filling out the First Report of Injury or Illness for the Florida Department of Financial Services Division of Workers’ Compensation, it is crucial to provide accurate and comprehensive information to ensure the proper handling of the claim. Here are key takeaways that one should consider:
- It is necessary to print or type the information clearly to avoid misunderstandings or processing delays.
- The form asks for detailed employee information, including name, Social Security Number, date of accident, time of accident, home address, and a description of the accident including the cause of injury.
- Employer information is also required, such as the company name, Federal ID Number (FEIN), the nature of business, policy/member number, and details if the employer will continue to pay wages instead of workers’ compensation.
- The form requires information on the injury or illness, including the part of body affected, the date of birth of the injured or ill employee, and their sex.
- Details related to the claims-handling entity need to be filled out, including whether the case has been denied or if it's a lost time case. This involves providing dates and details on disability, knowledge of the 8th day of disability, and if full salary was paid in lieu of compensation.
- The form includes a section for remarks, which can be used to add any additional information or clarification that might be helpful in processing the claim.
- An acknowledgment statement at the end of the form highlights the seriousness of submitting false or misleading information, indicating that it could be punishable as insurance fraud.
- Both the employee and employer signatures are necessary, verifying that they have reviewed, understood, and acknowledged the statements on the form. There is also a place for the employer to indicate whether they authorized the form.
Understanding each part of this form is essential for ensuring that the claims process is initiated correctly, thereby facilitating timely support and benefits for the injured or ill employee. It is a crucial document that requires thoroughness to avoid complications in the workers' compensation claim processing.
Popular PDF Templates
How to Make a Job Application Form - Enable a smooth transition into Florida state employment by meticulously filling out this application, which is your step towards a promising career.
Florida Homeschool Graduation Requirements - The process of filling out and submitting this form symbolizes a commitment to providing a comprehensive education outside the traditional school setting.